









Introduction
Haemorrhoidal disease (HD) is a common anorectal disorder and one of the commonest causes of bleeding per rectum [1]. Multiple treatment modalities are available for every grade of HD, including injection sclerotherapy, rubber band ligation (RBL), infrared coagulation, cryoablation, bipolar diathermy, and laser surgery (the so-called bloodless knife) [2–9].
Cryotherapy is not only time consuming, but also results in considerable discomfort to the patient [10]. RBL, although simple, has the drawbacks of post-procedural pain and slippage of the ligatures leading to increased recurrence [11]. Sclerotherapy is useful only in early cases, and the technique is associated with septic complications limiting its use in advanced HD [12, 13]. Complications like fissures, bleeding, and spasm are seen with bipolar probes [14]. Less invasive procedures such as haemorrhoidal artery ligation (HAL) are not cost effective [15], and stapled haemorrhoidopexy is associated with a 0–15% incidence of anal stenosis, precluding its use in mild to moderate cases [16]. Excision of HD is used nowadays only for complicated cases. Surgical procedures such as Milligan-Morgan haemorrhoidectomy require anaesthesia and in-patient stay, and result in postoperative pain that may require analgesic therapy, and the return to work usually takes about 1–2 weeks.
So, in present times, a procedure that is painless and rapid, and which can be performed on an out-patient basis, is always preferred. There is no single technique that is universally considered as best. Infra-red coagulation is unsuitable for grade 3 and grade 4 HD [17]. Radiofrequency ablation (RFA) utilizes an electrical current produced by radio waves to generate heat, and this has been studied previously for early-stage HD with promising results [6]. There are a few studies demonstrating the use of RFA for advanced HD. RFA overcomes the disadvantages of infrared coagulation, and this prompted us to use a newly developed probe that is operated at radio frequency (called Rafaelo®: “radio frequency of hemorrhoids in local anesthesia”), by F Care Systems, Antwerp, Belgium for the treatment of advanced HD.
Aim
The aim of the present study was to evaluate the efficacy and outcomes of the Rafaelo® technique for the treatment of HD.
Material and methods
Surgical procedure
After informed consent, all the patients were placed in lithotomy position under sedation anaesthesia. Local perianal block was given with total of 20 ml of 4.5 mg/ml solution of Ropivacaine, which was injected into ischiorectal fat immediately peripheral to the external sphincter (Figure 1). This injection targets the terminal nerve endings of the anus rather than blocking the trunks of major nerves.
Figure 1
Injection of local anaesthetic into the ischiorectal fat immediately peripheral to the external sphincter

A self-illuminating (LED), side-view proctoscope (69 mm × 23 mm) with 100 mm long handle was used for this procedure (F care systems, Antwerp, Belgium). This proctoscope has a simple vent on one side, through which a single haemorrhoidal tissue bulges out and the rest of the anal cushions are compressed so that one haemorrhoidal tissue can be tackled at a time.
A fluid barrier was created by injecting 3 ml of normal saline (NS) between the submucosa of haemorrhoidal tissue and the internal anal sphincter muscle (Figure 2). This step prevents heat transmission to the internal anal sphincter muscle, which can damage the sphincter, leading to postoperative pain.
Figure 2
A fluid barrier is created by injecting 3 ml of normal saline (NS) between the submucosa of haemorrhoidal tissue and internal anal sphincter muscle

An HPR 45i probe (F care systems, Antwerp, Belgium) with 4 MHz frequency was deployed into the haemorrhoidal tissue, and a continuous mode of radiofrequency ablation was used to coagulate the haemorrhoid.
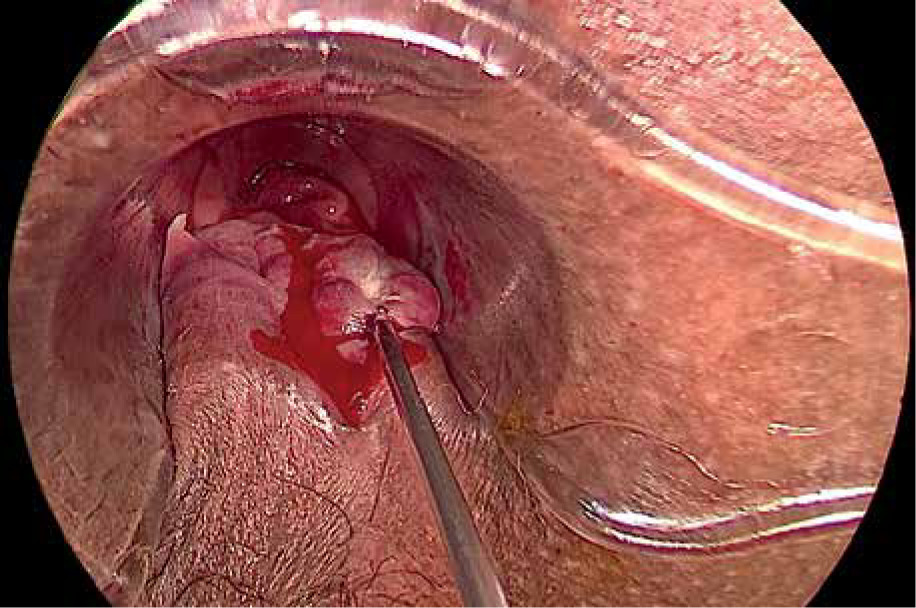
The tip of the RFA probe was inserted into the haemorrhoidal tissue proximal to the dental line, to a depth of about 5 mm, and the tissue was gently lifted before delivering the radiofrequency (RF) current (Figure 3). The RF application was continued until the haemorrhoidal tissue exhibited whitish discoloration (Figure 4). After withdrawal of the probe the puncture site was sealed with application of the RF probe to ensure haemostasis. A power setting of 25 W (maximal temperature development of 125–130°C) was used per haemorrhoidal mass with total energy of up to 2500 J as per the local anatomy. In order to cool down the treated area a cold saline-soaked gauze piece was applied immediately to the surface of the haemorrhoidal tissue.
Figure 3
The tip of the RFA probe is inserted into the haemorrhoidal tissue proximal to dental line, to a depth of about 5 mm, and the tissue was gently lifted up before delivering the radiofrequency current

Figure 4
The RF application is continued until the haemorrhoidal tissue exhibits whitish discoloration
Finally, the haemostasis was confirmed, and any bleeding spots were coagulated with the probe tip. Two-finger anal dilatation was done in all cases to cause symptomatic relief of anal spasm. An anal pack, which was lubricated with 2% lignocaine jelly and povidone iodine ointment, was inserted into the anal canal. This pack was removed a few hours later or upon the urge for defecation. After pack removal the patients were advised to have a warm water sitz bath and topical application of anaesthetic jelly as per the requirement for pain relief. All patients were given oral analgesics for up to 1 week. A post-procedural check examination was done on post-operative days (POD) 3 and 7, and at 2 months (Figure 5).

Study design
We carried out a retrospective observational study in patients admitted at a tertiary care centre from June 2019 to December 2020. Patients who were above the age of 18 years and under 80 years with grade 2, grade 3, or grade 4 HD were included in the study. All patients had previously failed the conservative treatment for HD. All patients were operated by a single surgeon at a single centre. Pregnant and lactating mothers, patients with rectal prolapse/on anticoagulants/with pacemakers/with anal cryptitis, proctitis, or fissure-in-ano and patients with history of anal or rectal carcinoma were excluded.
Data collection
The dataset included patient demographics, American Society of Anesthesiologists (ASA) score [18], details of the procedure, and complications if any. The haemorrhoidal severity score (HSS) [19] was calculated for the patients prior to the procedure and 2 months after. The Cleveland Incontinence Score (CIS) [20] was used to assess the quality of life of the patients due to incontinence prior to and 2 months after the procedure. The Visual Analogue Score (VAS) for pain was calculated on POD 3 and 7.
Results
Patient characteristics
A total of 47 patients were included in this study. There were 38 (80%) males, and the mean age of this cohort was 43 years (range: 26–57 years). All the patients had an ASA score of less than 2. There were 20 (42.5%) cases of grade 2 HD, 17 (36%) cases of grade 3, and 10 (21.5%) cases of grade 4 HD in the present cohort. All the patients had failed conservative management for HD in the past, with 9 cases giving a history of RBL (Table I).
Table I
Patient demographics (n = 47)
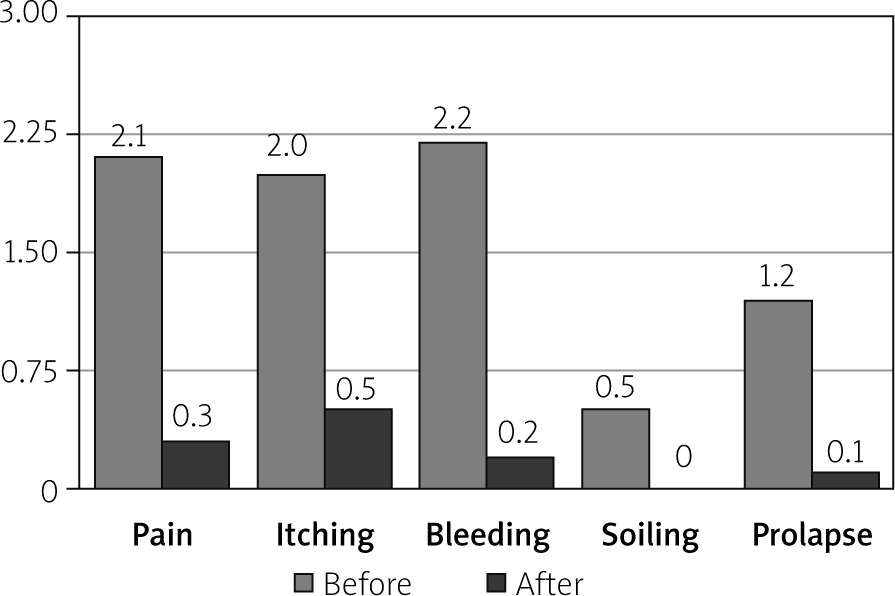
Haemorrhoidal Severity Score (HSS)
The mean HSS score prior to the procedure was 8.31 ±2 which improved to 1.12 ±1. We noted a statistically significant improvement in all individual symptom scores of HSS (Table II, Figure 6). Minor post-operative bleeding was noted in 6 (12%) patients in the first 2 weeks. It occurred between days 5 and 13 of the procedure. This bleeding was associated with defecation, and reassurance was all that was necessary. Three (6%) patients had significant bleeding. They were managed conservatively with local haemostatic compression, and all the patients had an uneventful recovery. Ten (20%) patients had complaints of mucous discharge from the anus, soiling the underclothes for 5 to 10 days. No specific treatment was given, and the discharge stopped spontaneously within 2 weeks. No patients complained of soiling at 2 months. Twelve (25%) patients had itching in the perianal region, which was treated with local lubricant jelly. Itching was the most common complaint at the end of 2 months.
Pain and Cleveland Incontinence Score
Five (10%) patients complained of pain in the anal region. The mean VAS score was 3 on POD 3 and 1 on POD 7. Patients were treated with NSAIDS, and no patient required analgesics beyond 1 week. Three patients had complaints of incontinence prior to the procedure. The mean CIS was 0.2, with all 3 patients having a CIS of 3. Subsequently, all the patients had a score of 0 post procedure.
Complications and follow-up
There were 3 instances of urinary retention in the post-operative period, which required urinary catheterization (Table III). No infective complications were noted in this study. Three patients had recurrence of HD at 2 months, and all were recommended to undergo a second Rafaelo® procedure. Anal stenosis was not observed in any patients at 2-month follow-up. Patients were comfortable, and the majority (56%) had a return to normal activity within 4 days of the procedure.
Discussion
An ideal treatment for HD would be a method that returns the anal cushions to their normal size without destroying them or damaging the surrounding tissues that are responsible for continence. The radiofrequency electrode, in contrast to the diathermy electrode that works at a frequency of 0.5–1.5 MHz, remains cold at application because of the use of very high-frequency radio waves delivered at 4 MHz [8, 21]. These high-frequency waves heat the tissue under treatment thereby causing haemostasis [17, 21]. RFA leads to an immediate reduction in blood flow to the haemorrhoids followed by fibrosis and scarring of the wound. This leads to tethering of the mucosa to the underlying tissue, preventing haemorrhoidal prolapse [6, 17]. Furthermore, the atraumatic nature of RFA minimises the postoperative sequelae, such as pain, blood loss, and local tissue oedema [21].
This procedure is safe and easy to perform with a small learning curve. Coagulation of the haemorrhoid occurs rapidly (usually within 5–10 s), and because the pile mass is directly coagulated, it facilitates immediate disappearance of the haemorrhoid under vision. Unlike photocoagulation, the RFA probe does not have a ‘cool down’ period, which makes the procedure quicker and more comfortable for the patient [22]. RFA can also be used safely without antibiotic cover because the RF current provides sterilization while in use. Moreover, the RF coagulated area is aseptic, and the necrotic zone formed by heat coagulation of haemorrhoids is impenetrable by bacteria [23].
In agreement to previously published literature, we also noted a statistically significant improvement in the HSS within 2 months of the procedure [24]. All the patients noted a complete recovery from soiling of the underclothes in this study. Pain and bleeding were the predominant complains of the patients prior to the procedure, and significant resolution was seen in both the symptoms after the Rafaelo® procedure. Complaints of itching showed the least improvement amongst the HSS individual symptom scores. All complaints of itching were managed by local application of lubricant jelly on an out-patient basis and were not associated with significant discomfort to the patient.
RFA ablation for HD was initially described by Gupta [6] in 2002. The technique was described for early-stage HD, and Gupta reported excellent results. The group also compared this technique with RBL for treatment of grade 2 HD and noticed lower pain and lower recurrence rates. However, the incidence of bleeding and prolapse was higher in the RFA group in that study [25]. This led to other authors using this technique even for advanced HD [24, 26]. Eddama et al. recently employed this technique in the National Health Service (NHS) for grade 3 and grade 4 HD and reported promising results [24]. Our study was conducted in a low-middle-income country with very different population characteristics, with many patients having a delayed presentation to the hospital. We were able to produce equivalent results to previous published literature, and this may validate the addition of RFA to the armamentarium of surgeons treating advanced HD.
There were no serious complications and no instances of damage to the sphincter complex in this study. Instilling cold saline between the submucosa of the haemorrhoidal tissue and internal anal sphincter helps in dissipating the heat, which protects the underlying muscle from necrosis. This technique may explain the perfect continence (CIS score of 0) observed in the post-operative period in this cohort. We also routinely performed anal dilatation for all the patients, which reduced the post-procedural anal spasm and led to lower pain scores in our cohort. All the patients in our cohort returned to normal activity within 1 week, with 56% of the patients claiming full recovery in just 4 days. We preferred sedation in all our cases in addition to local anaesthesia because this was our initial experience with the use of the Rafaelo® technique, but we intend to use only a local anaesthesia block in our future cases for faster recovery and early return to work.
A small sample size and lack of a control group limit the application of this study. It is a single-arm study in which the patients were managed by a single experienced surgeon in a high-volume referral centre. This may constitute a bias because it is unclear whether or not similar results would be produced by a less experienced surgeon. A longer follow-up is also required to prove the robustness of the treatment. The capital investment to purchase an RFA probe is high, but the running costs are minimal. A detailed analysis of health economics was not performed in this study.
Conclusions
The Rafaelo® technique is a safe and effective treatment alternative for advanced HD. It results in a statistically significant improvement in the symptoms of HD and is associated with minimal discomfort to the patient with early return to normal activity. We did not see any major complications with this procedure and would advocate its use in HD. Future randomized controlled studies comparing Rafaelo® to other treatment modalities are recommended to assess the long-term reliability and efficacy of this procedure.