









Introduction
Colon cancer, especially colon adenocarcinoma, is traditionally regarded as the most commonly diagnosed gastrointestinal malignant disease. Nevertheless, despite advances in diagnosis and novel therapeutic options, the clinical outcomes of colon cancer patients with locally advanced or metastatic disease are still not satisfactory. The patients’ overall survival (OS) is largely dependent on the disease stage at the time of diagnosis and/or surgical resection [1, 2]. Importantly, approximately 20% of the diagnoses are made in the metastatic stage of the disease. In this case the 5-year overall survival is less than 15%. Importantly, the prognoses are not satisfactory even in the case of patients with primary tumors. Therefore, the identification of novel approaches for describing the patients from the high-risk group, particularly in the context of the clinical outcomes, has become a major challenge [3, 4].
The Notch signalling pathway is an evolutionarily conserved cell signalling mechanism involved in a wide array of cellular processes. Among them should be mentioned proliferation, differentiation, apoptosis, and stem cell maintenance. It is generally accepted that there are 4 Notch receptors: Notch1, 2, 3, and 4, which are synthesised as precursors composed of extracellular, transmembrane, and intracellular domains. Within the cisterns of the Golgi complex, the precursors of Notch receptors are cleaved by furin-like convertases to generate 2 subunits. One subunit contains most of the extracellular domain, and the second subunit consists of the rest of the extracellular and transmembrane domains. The Notch ligands comprise 5 members: Jagged1/2 and Delta-like 1/3/4 (DLL1/3/4). All these ligands are single-pass type I transmembrane proteins. The extracellular domain of the Notch receptor has been shown to contain 36 EGF-like repeats [5, 6]. Ligand binding to EGF-like repeats unfolds the negative regulatory region (NRR), permitting the next cleavage by metalloproteases of the ADAM family. During the next step, γ-secretase complex executes an intramembrane cleavage releasing the Notch intracellular domain (NotchIC or NICD), which translocates to the nucleus [7, 8]. It has been demonstrated that for activation of the Notch signalling the Mastermind-like family of proteins (MAML1/2/3) are needed. MAML forms a ternary complex with CBF1 (Centromere-binding protein 1) NotchIC by direct interaction with NotchIC. Then, the ternary complex composed of CBF1-NotchIC-MAML acts as a transcriptional activator, leading to Notch target gene transcription. Among the primary targets there are several genes belonging to the basic helix-loop-helix (bHLH) family. Following Notch activation, at least 2 families of bHLH proteins are induced: the Hairy/Enhancer-of-Split (HES) family and the Hairy-Related Transcription factor (HRT) family, which are known to be transcriptional repressors [1].
Notch signalling has been revealed to be involved in the pathogenesis of gastrointestinal tumours such as gastric and colon cancer. Similarly to the differentiation process, its effect during carcinogenesis is probably cell type specific and circumstance dependent. Expression of Notch3 protein has been revealed to be upregulated in Asian colon cancer patients [1, 2, 9]. Thus, it remains to be determined whether those findings are applicable to Caucasian patients and finally to the general population with colon cancer, especially those with colon adenocarcinoma.
Aim
The current study investigated the expression of Notch3 protein in Caucasian patients with colon adenocarcinoma to assess its prognostic significance by correlating its expression with the clinicopathological variables and overall survival (OS).
Material and methods
Tissue samples
All colon adenocarcinoma samples were collected from patients who underwent radical surgery at the Municipal Hospital in Jaworzno. All patients were definitively diagnosed with colon adenocarcinoma and did not receive adjuvant chemotherapy, radiotherapy, or immunotherapy prior to surgery. The exclusion criteria were as follows: (1) history of previous malignant disease, (2) familial adenomatous polyposis, (3) inflammatory bowel disease, (4) preoperative anti-cancer treatment, and (5) evidence of distant metastasis. The clinicopathological characteristics obtained from the medical records were as follows: age, gender, location of tumour, grade of tumour differentiation, depth of invasion, regional lymph node involvement, operation record, treatment record, reoccurrence, and vital status at the last follow-up date.
The colon adenocarcinoma specimens belonged to 48 men and 49 women (mean age: 68; range: 33–89 years). Tumours were located in the proximal part of the colon in 50 (51.5%) cases and in the distal part of the colon in 47 (48.45%). Three levels of differentiation were used to classify the grading as follows: well differentiated (G1), 14 (14.43%) cases; moderately differentiated (G2), 52 (53.61%) cases; and poorly differentiated (G3), 31 (31.96%) cases (Table I).
Table I
Demographic, clinical, and tumour-related characteristics of patients included in the study (n = 97)
Immunohistochemical staining
For the immunohistochemical studies the paraffin-embedded specimens were cut into 4-µm-thick sections, fixed on Polysine slides, and deparaffinised in xylene and rehydrated through a graded series of alcohol. To retrieve the antigenicity, the tissue sections were treated twice with microwaves in a 10 mM citrate buffer (pH 6.0) for 8 min each. Subsequently, sections were incubated with rabbit polyclonal antibody to Notch3 (final dilution 1 : 600) (Abcam cat. number ab23426). For visualisation of protein expression, the sections were treated with the BrightVision detected system and Permanent AP Red Kit (Zytomed). Mayer’s haematoxylin was used to counterstain the nuclei.
The scores were assigned separately for the stained area and for the intensity of the immunohistochemical reaction. Quantification connected to the stained area of the tissue section was performed as follows: (1) < 33% of cells showed immunoreaction, (2) 33–66% of the cells had positive reaction to Notch3, and (3) > 66% of the cells were positive. The intensity of the immunohistochemical reaction was quantified as follows: (1) absent or weak, (2) moderate, and (3) strong. Each tissue section was characterised by a final grade derived from the multiplication of the stained area and the intensity of the staining. The Notch3 expression was considered to be absent/low for grade 1; moderate for grades 2, 3, and 4; and strong for grades 6 and 9.
Statistical analysis
Statistical analyses were conducted using Statistica 9.1 (StatSoft, Poland). The clinical characteristics of the patients in relation to Notch3 immunoreactivity were assessed by performing the Kruskal-Wallis test and U Mann-Whitney test. The Kaplan-Meier method was used to study survival curves and the long-rank test to compute differences between the curves.
Results
To investigate the prognostic role of Notch3 expression, the immunohistochemical analysis was performed in colon adenocarcinoma tissues and adjacent non-pathological colon tissues in patients with colon adenocarcinoma. It should be noted that expression of this protein in non-pathological samples was described as weak or moderate. In samples of colon adenocarcinoma, the high, moderate, and weak level of Notch3 protein was revealed (Figure 1). Among the 97 colon adenocarcinoma samples, 11 (11.34%) showed weak immunohistochemical reaction, 35 (36.08%) demonstrated moderate immunoreactivity, and 51 (52.58%) revealed strong expression. The relationships between the Notch3 levels and each clinicopathological parameter are summarised in Table II.
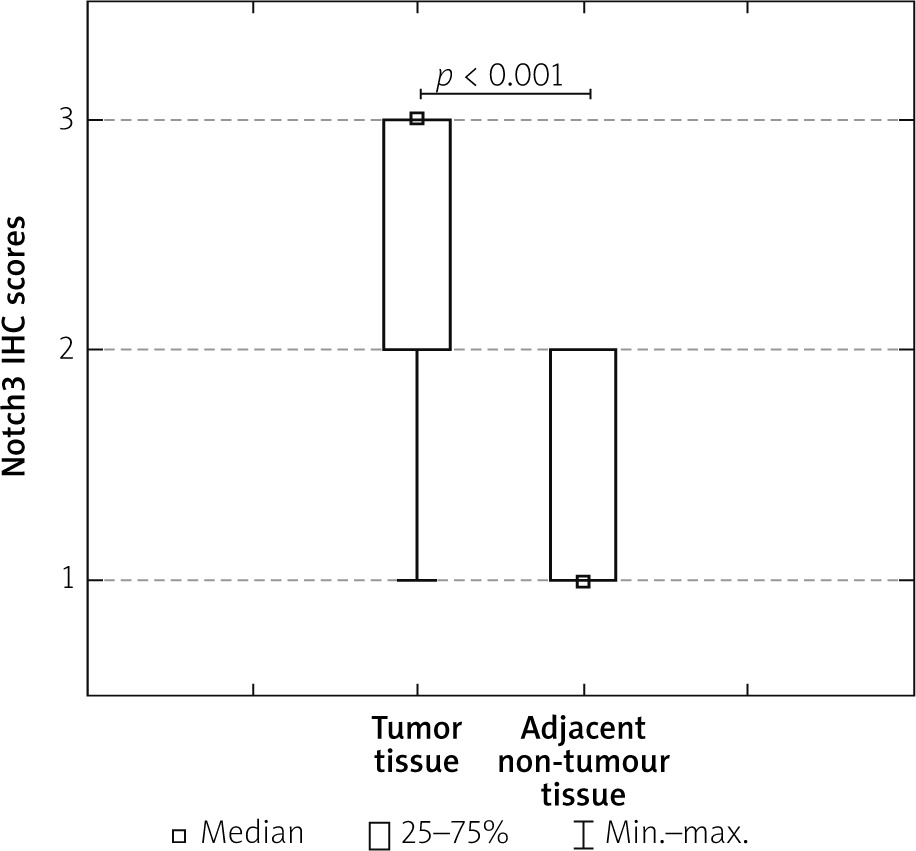
Table II
Correlations between Notch3 immunoexpression and clinicopathological characteristics in colorectal cancer patients
As demonstrated, the level of the Notch3 immunohistochemical reactivity was correlated with the grade of the histological differentiation (p < 0.001). A strong expression of Notch3 protein was detected more frequently in patients with G3 tumours than in patients with G1 tumours. Moreover, a significant difference was also found between the patients with G1 tumour and those with G2. In the G2 patients a strong reactivity was described more frequently. The statistical evaluation of Notch3 immunoexpression according to age, sex, tumour location, and depth of invasion revealed no significant difference among these variables (all p > 0.05; Table II).
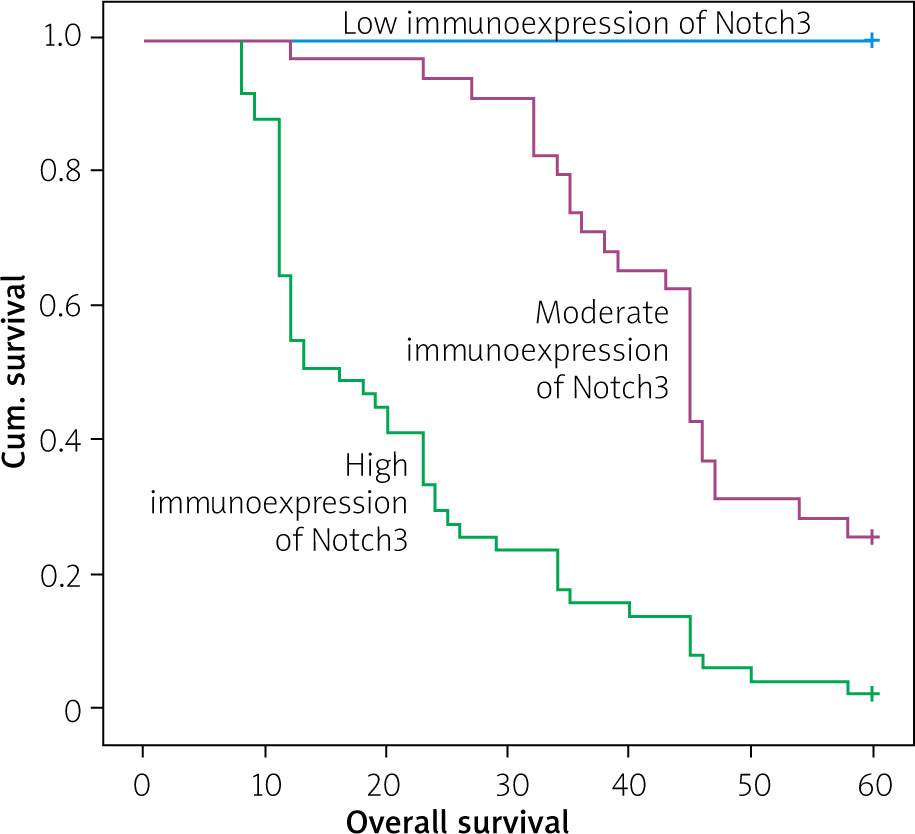
The Kaplan-Meier survival analysis showed that the overall survival rate in the group of patients with a low expression level of Notch3 was significantly longer than that for patients with a moderate or strong level of Notch3 immunoreactivity (p < 0.001; Figure 2). The 5-year overall survival for patients with a low, moderate, or strong level of Notch3 immunoexpression was 100%, 25.7%, and 2%, respectively. The Notch3-moderate patients had an average survival time of 44.886 months (95% CI: 40.855–48.916), whereas the Notch3-strong expression groups had an average survival time of 21.706 months (95% CI: 17.863–25.549). In the univariate analysis the grade of tumour differentiation and Notch3 immunoexpression were found to be significantly associated with reduced 5-year survival. Moreover, a multivariate analysis demonstrated that grade of tumour differentiation (HR = 2.150; 95% CI: 1.380–3.349, p = 0.001) and Notch3 expression (HR = 3.901; 95% CI: 2.436–6.247, p < 0.001) were also independent risk factors for worse survival (Table III, Figure 3).
Figure 2
Immunohistochemical expression of Notch3 protein in tumour tissue: A, B – control, C, D – weak expression of Notch3 protein in colon adenocarcinoma samples, E, F – moderate expression of Notch3, G, H – strong expression of Notch3 (C, E, G – 25×; D, F, H – 100×)
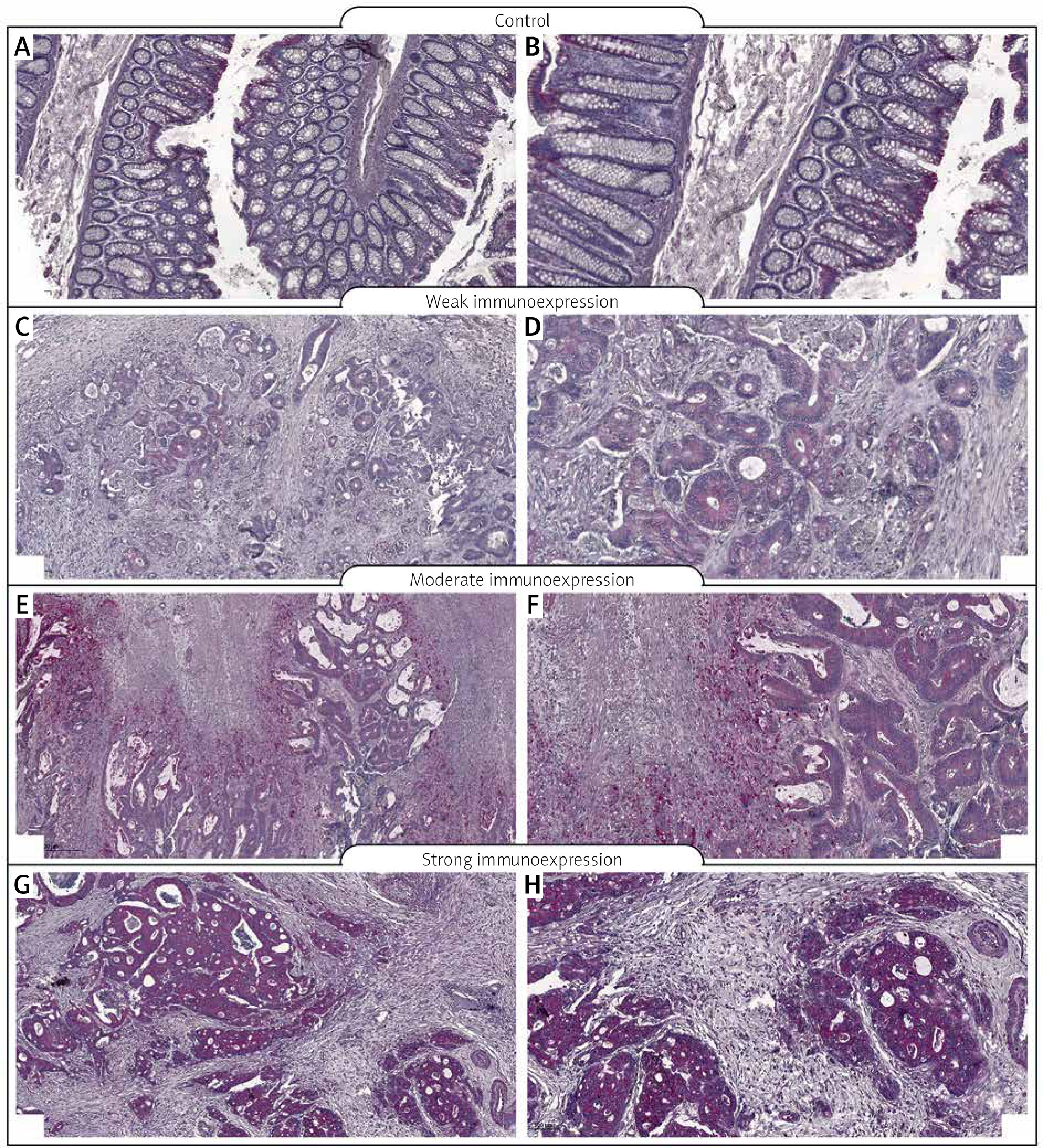
Table III
Univariate and multivariate analyses of various prognostic parameters in colorectal cancer patients using Cox regression analyses
Discussion
The results of our study demonstrate that in comparison to samples of non-tumour colon mucosa, the tissues of colon adenocarcinoma were characterized by a high level of Notch3 immunoreactivity. Furthermore, the high level of Notch3 immunoexpression was demonstrated to be associated with the malignancy-related clinicopathological factors and 5-year overall survival of patients. The high immunoexpression of Notch3 was significantly related to advanced histological tumour grade. The Kruskal-Wallis test showed a statistical difference between the patients with G1 tumours and those with G2 tumours, and between the patients with G1 tumours and those with G3 tumours. In both cases, patients with G1 tumours were described by a low level of Notch3 immunoexpression (p < 0.001).
As revealed by the studies, a high level of Notch3 accompanied by a positive correlation with the expression of JAG1 and JAG2 was observed in serous ovarian carcinomas. Moreover, the high expression of Notch3 was significantly associated with advanced stage, lymph node metastasis, chemoresistance, and poor overall survival [10]. In recurrent ovarian carcinoma, increased level of Notch3 nuclear expression also demonstrated a correlation with poor clinical prognosis [11]. Ectopic expression of Notch3 following transduction with NICD3 in ovarian surface epithelium and low-grade serous ovarian cancer cells is associated with increased resistance to carboplatin during in vitro conditions. The activation of Notch3 in OVCA429 cells was responsible for a fibroblast-like morphology and induction of the smooth muscle α-actin, Slug and Snail. Interestingly, decreased expression of E-cadherin was observed. This may suggest that Notch3 activation generates epithelial-to-mesenchymal transition (EMT). Interestingly, Notch3 activation rendered OVCA429 cells more resistant to carboplatin-induced cytotoxicity and impaired carboplatin-induced apoptosis [12, 13]. Some authors revealed that Notch3 is highly expressed in colon cancer. Nuclear expression of Notch3 has been correlated with tumour recurrence and may serve as a novel predictive marker in recurrent stage II and III colorectal cancer [14]. Notch3 signalling also induced the expression of Cdc42- and Rac1-specific guanine nucleotide exchange factor Asef in cancer cells. Furukawa et al. revealed that mutant APC and Notch3 might cooperate to cause Asef-mediated aberrant colorectal tumour cell migration and adenoma formation [15]. In colon cancer, forced expression of Notch3 increased the level of MUSASHI-1 (MSI-1). In contrast, the silencing of Notch3 by shRNA reduced the MSI-1 level in both colorectal cancer cells and tumour xenografts. Moreover, enforced Notch3 expression or stimulation by DLL4 enhanced levels of Notch1 in colorectal cell lines [16]. In lung cancer cell lines, Notch3 was also upregulated, and it was associated with karyotypic abnormalities [17]. In NSCLC this receptor was abundantly co-expressed with EGFR to promote lung carcinogenesis [18, 19]. Notch3 is known to have a crosstalk with the EGFR-mitogen-activated protein kinase pathways, leading to suppression of apoptosis through BIM activity [20]. In the study by Yuan et al. a combined analysis of 19 eligible clinical studies demonstrated a predictive value for Notch1 and Notch3 expression in NSCLC patients. The results of the meta-analysis suggest that expression of Notch3 is related to lymph node metastasis. This suggests that overexpression of Notch3 has a prognostic value for overall survival [21].